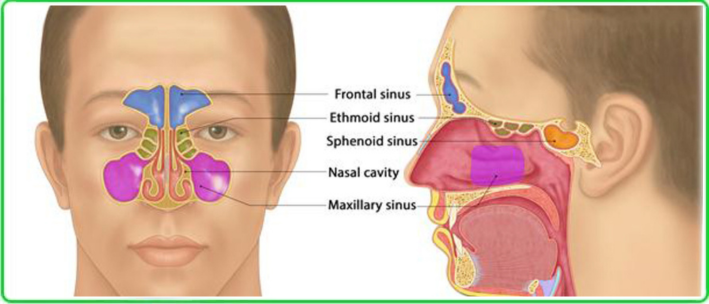
The maxillary sinus is often called the “antrum of Highmore,” named after the British surgeon and anatomist Nathaniel Highmore (1613–1685), who first described it in detail more than 350 years ago. Inflammation of the lining of this sinus is still commonly referred to as sinusitis.
In the past, sinusitis was seen as an almost inevitable consequence of a cold. The paradox today is that the most frequent cause of sinusitis is still the common cold, triggered by respiratory viruses.
Why Does a Simple Cold Sometimes Turn Into Sinusitis?
A viral cold depends on the immune system.
- In some people, the immune defenses quickly neutralize the virus. Nasal congestion lasts about a week and resolves without complications.
- In others, factors such as weakened immunity, chronic diseases, structural features of the nose and sinuses, smoking, or incorrect treatment of a cold increase the risk of sinusitis.
This is when a seemingly harmless cold turns into a bacterial sinus infection.
How to Recognize Sinusitis
Stagnant mucus and swollen nasal mucosa block drainage and create favorable conditions for pathogens. Only an ENT specialist can reliably distinguish sinusitis from a prolonged cold — especially when symptoms occur for the first time. The gold standard for acute sinusitis (acute rhinosinusitis) diagnosis includes:
- Clinical presentation: symptoms lasting longer than 10 days without improvement, or “double worsening” after initial relief.
- Nasal endoscopy: visualization of purulent discharge in the middle meatus.
- Sinus ultrasound: quick, non-invasive, and safe (particularly in children and pregnant women), though less sensitive than CT.
- CT scan of the paranasal sinuses (axial and coronal views): highly sensitive for detecting mucosal thickening, fluid levels, and obstruction.
- Microbiological testing in severe cases, to identify the pathogen and guide antibiotic therapy.
Preparing for an ENT Consultation
To make your consultation most effective, record your symptoms in advance.
Checklist:
- Duration and severity of nasal congestion and breathing difficulty.
- Type of nasal discharge (clear, purulent, one- or both-sided).
- Facial pain or pressure in the cheeks, teeth, or nasal bridge, especially when bending forward.
- Headache radiating to the forehead or back of the head.
- Loss or reduction of smell.
- Fever, malaise, or signs of intoxication.
In children: sinusitis often manifests as persistent cough (especially at night) and may be associated with adenoiditis(mouth breathing, snoring, restless sleep).
Bring notes about when symptoms first appeared, how they changed over time, which medications were tried, and what effect they had. This will help your doctor reach the correct diagnosis faster.
When to Seek Urgent Medical Help
Sinusitis can sometimes cause dangerous complications. Seek immediate care if you notice:
- Eye problems: double vision, sudden vision loss, eyelid swelling or redness.
- Severe headache: unbearable, one-sided, worse with movement.
- Facial swelling or asymmetry with redness or deformation.
- High fever (above 38.5–39 °C) that does not improve with standard treatment.
- Neurological signs: neck stiffness, nausea, vomiting, confusion.
- Severe general deterioration despite ongoing therapy.
Clinical Case Scenarios
Post-viral sinusitis
Anna, 28, office worker. After a viral infection, she has persistent nasal congestion and mild headache for 7 days. No fever, clear discharge. Diagnosis: mild post-viral sinusitis (prolonged cold). Treatment: nasal irrigation with saline or ozonized water; intranasal corticosteroid spray.
Acute bacterial sinusitis
Sergey, 36, driver. Cold symptoms improved, then worsened: purulent discharge, left cheek pain, fever 38.2 °C, symptoms persisting for 12 days. Diagnosis: acute bacterial sinusitis (left). Treatment: amoxicillin/clavulanate for 7–10 days; mometasone nasal spray; nasal irrigation.
Severe sinusitis with complication
Irina, 45, teacher. Severe right-sided facial pain, eyelid swelling, fever 39.3 °C, double vision. Diagnosis: complicated bacterial sinusitis with orbital involvement. Treatment: urgent hospitalization; IV ceftriaxone; ophthalmology consult; sinus puncture and irrigation.
Chronic recurrent sinusitis
Dmitry, 52, construction worker, smoker. Multiple yearly flare-ups for 2 years: constant congestion, cough, reduced smell. Diagnosis: chronic recurrent sinusitis. Treatment: CT scan + endoscopy; conservative therapy during the acute episodes (antibiotics, nasal steroids, irrigation); planned endoscopic sinus surgery (FESS).
Common Questions
Can I use decongestant nasal drops?
Not as a treatment. They should only be used briefly, as prescribed by a doctor. Overuse leads to permanent damage to the nasal mucosa and addiction-like dependence.
Do folk remedies help?
No. At best, they are ineffective; at worst, they can cause severe intracranial or orbital complications.
Prevention of Sinusitis
- Treat viral infections on time.
- Address chronic infection sources (tooth decay, tonsillitis).
- Control allergies.
- Maintain good nasal hygiene and humidify indoor air.
- Get vaccinated against influenza and pneumococcal infection.
Sinusitis Treatment at KindCare Medical Center
At KindCare Medical Center, we provide modern diagnosis and treatment for all forms of sinusitis in adults and children:
- Endoscopic examination of the nose and sinuses.
- Ultrasound of the paranasal sinuses.
- CT scans for detailed assessment.
- Individualized medication therapy.
- Minimally invasive procedures (sinus puncture, endoscopic surgery).
- Long-term management of chronic rhinosinusitis.
Our specialists:
- Dr. Maryna Kryshtopava — ENT specialist, PhD, Associate Professor, with over 23 years of experience, expert in endoscopic diagnostics and sinus surgery.
- Dr. Irina Ivanova — pediatrician with more than 25 years of experience, specialized in ENT disorders in children.
- Dr. Timur — neurologist with 15+ years of experience, focused on neurological complications of sinus disease.
At KindCare, we ensure a multidisciplinary approach: ENT + pediatrician (for children) + neurologist (for complications). This team-based method minimizes risks and speeds recovery.
Nathaniel Highmore first described the maxillary sinus — today, we preserve its health at KindCare!